Trismus or limited mouth opening is a major complication of oral cancer. Radiation therapy is crucial in treating oral cancer, but in the long run, it leads to fibrosis, trismus and muscular stiffness that restricts oral functions. In advanced cases, Trismus Correction surgery is the only option. Other options available for treatment are the release of fibres and reconstruction using local flaps.
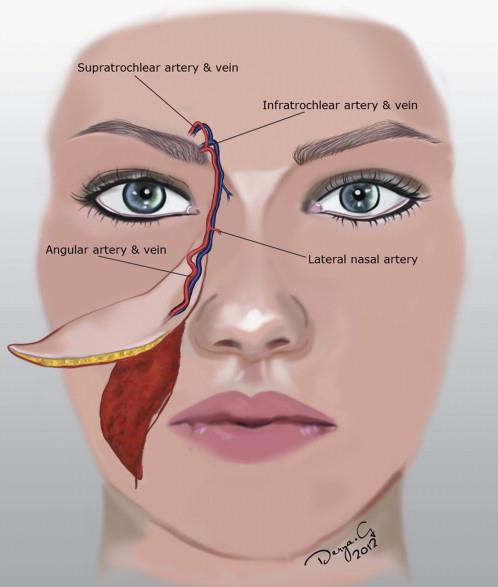
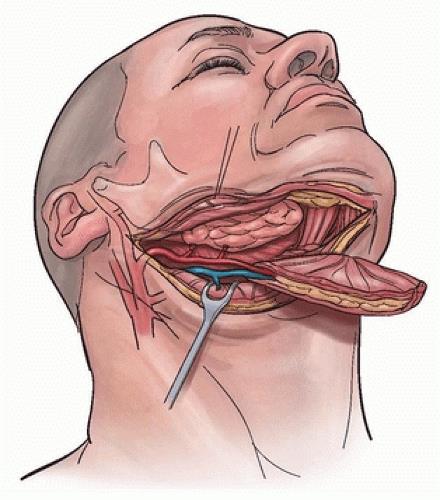
Over the last 2 decades, it has become popular as a reliable choice in the reconstruction of oral cavity defects and in trismus correction post-radiation therapy. It is an axial pattern skin flap based on the submental artery, a consistent branch of the facial artery.
The submental island flap has shown promising results due to its versatile use, wide arc of rotation, excellent color match, low donor site morbidity, and effectiveness in trismus correction post-radiation therapy.
Deltopectoral Flap
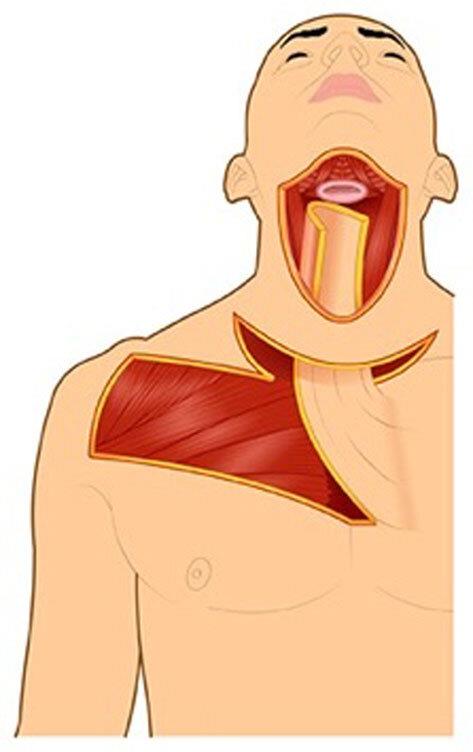
The deltopectoral (DP) flap represents a reconstructive option for the head and neck and can be effectively used in trismus correction post-radiation therapy. It is a skin and muscle flap raised from the anterior chest wall below the clavicle. Its role partially declined with the rise of free flaps. However, it still remains a valid option in patients who cannot undergo reconstruction with free flaps. It is known for its reliable anatomy, good colour matching with the facial skin, and texture. It is easily handled by a surgeon with lower failure rates.
Key aspects of the deltopectoral flap:
Indications:
It is used to reconstruct defects in the head and neck, those caused by tumour removal or fistulas (abnormal connections) or defects after trismus release, particularly in trismus correction post-radiation therapy. Specifically, it is used for:
-
Reconstruction of the cheek, oral cavity, pharynx, and neck
-
Covering exposed vessels or fistulas in the neck
-
Serving as a “backup” flap for failed free flaps or other reconstructive procedures
Advantages:
-
Reliable: The flap has a predictable anatomy and blood supply.
-
Good Colour Match: The skin of the flap often provides a good colour and texture match with the facial skin.
-
Ease of Harvesting: It can be harvested relatively quickly and easily.
-
Can be Delayed: This flap can be harvested in stages to increase its length and reach.
-
Can be Returned: The pedicle (blood supply) can be divided and returned to the donor site after a period of time, minimizing donor site morbidity, which is particularly helpful in trismus correction post-radiation therapy.
Surgical Technique:
-
The flap is outlined on the chest and shoulder region, including the deltopectoral groove.
-
Skin and subcutaneous tissue are elevated while carefully preserving the blood vessels.
-
The flap is then rotated or transposed to the recipient site.
-
The donor site is covered and sutured, often with a skin graft, to ensure proper healing and functionality, especially in cases like trismus correction post-radiation therapy.
Modern Considerations:The DP flap offers versatility in head and neck reconstruction. Depending on the tissue volume needed, the distance from the donor site, and patient-specific factors, this flap can be adapted to achieve optimal functional and aesthetic outcomes, particularly in trismus correction post-radiation therapy.
Anterolateral Thigh Flap
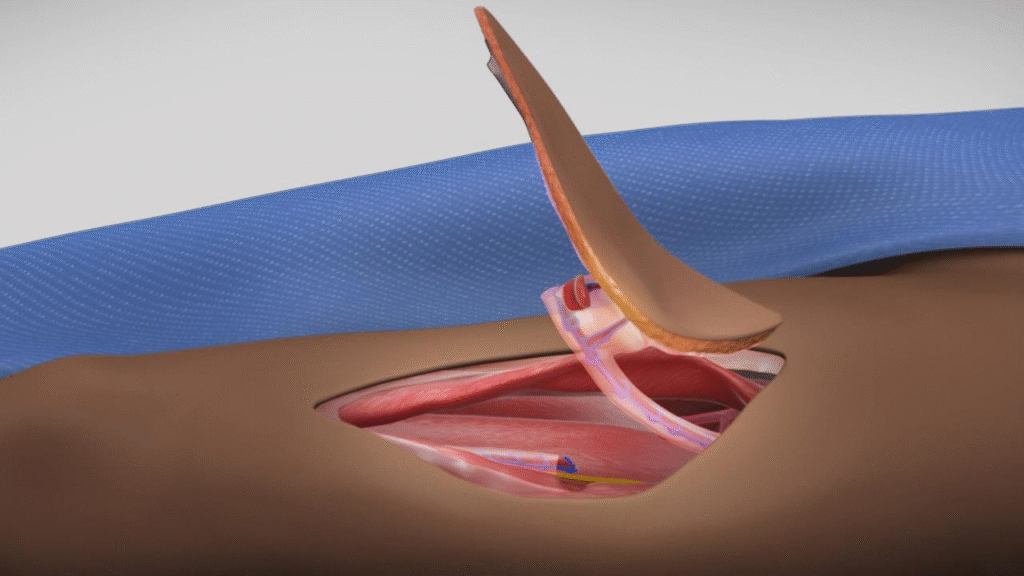
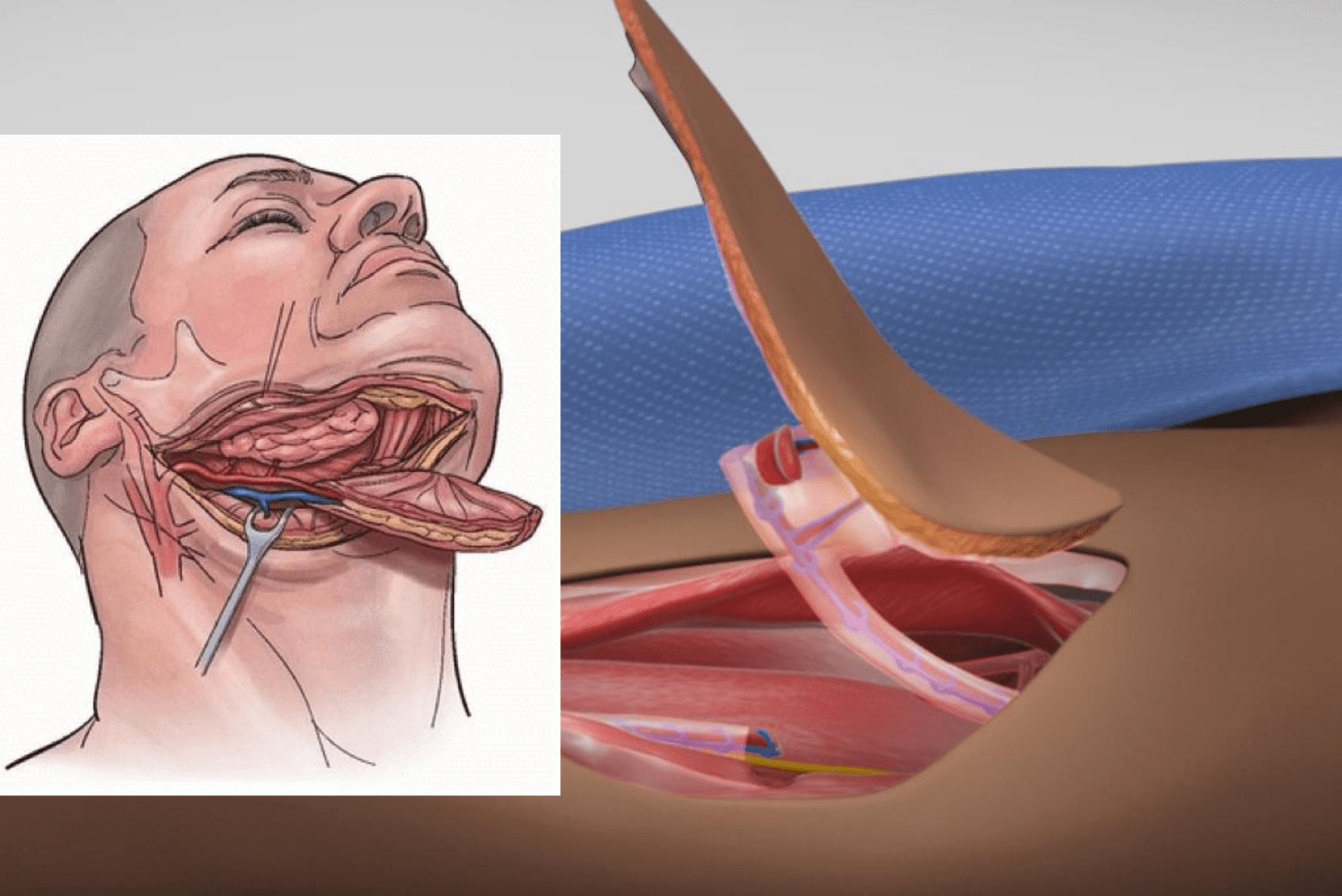
To cover the defects created on the face, a patch of skin, along with the fat and sometimes even muscle, from the front and outer part of your thigh is taken to replace the missing tissue elsewhere. The anterolateral thigh (ALT) flap allows for healthy, reliable, vascularized, soft-tissue coverage of defects of traumatic or acquired deformities. It can be used to cover defects created after trismus correction post-radiation therapy or mandible resection to aid in mouth opening.
The ALT flap was described by Song et al., which is based on blood supply emanating from the descending branch of the lateral femoral circumflex artery, which is present in the thigh region.
The magic behind the ALT flap lies in its blood supply. Your skin, muscles, and tissues are supplied by the network of blood vessels called perforators. One such perforator that supplies blood to this flap lies in the thigh and is a branch of the lateral femoral circumflex artery.