Introduction
RECONSTRUCTING A COMPLEX CASE OF BILATERAL TEMPOROMANDIBULAR JOINT ANKYLOSIS WITH PATIENT- SPECIFIC IMPLANTS
Here is a fascinating case of bilateral temporomandibular joint ankylosis- a condition that is a common occurrence but remains undiagnosed due to the lack of knowledge about the joint.
Temporomandibular Joint Ankylosis
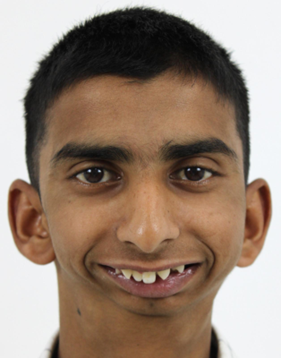
Let us take you through the journey of this young 18 year old boy who had come to us with a complaint of reduced mouth opening and a very short lower jaw. He has had this condition since childhood and has difficulty in eating food and talking and more sadly, has been a victim of bullying at school along with the other functional difficulties mentioned before.


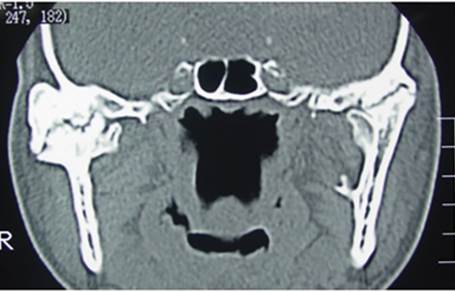
We asked him to get a preliminary CT scan to confirm our suspicion that showed a classical picture of fusion of the joint to the skull base.

Most patients do not know what a temporomandibular joint is and what its function is ! Like any other joint in the body, this joint connects the lower jaw to the skull and helps in opening and closing of the mouth. We can feel it if we place our fingers in front of the ear and open /close our jaw. If you feel only the joint and do not experience any clicking joint noises, then you can consider yourself lucky, as most of us might have clicking sounds without our knowledge. This usually happens because of multiple factors, but the most common being an improper bite.
However, in our case represented here, this patient gave us a history of trauma while playing in childhood where he fell from a tree directly on his face. This blunt, direct trauma to the joint caused its enlargement and fusion to the skull. This in turn led to the restricted mouth opening. Trauma to the joint is the most common reason for temporomandibular joint ankylosis. The other causes include spread of infection from the ear, inflammatory diseases, chronic inflammation and developmental conditions.
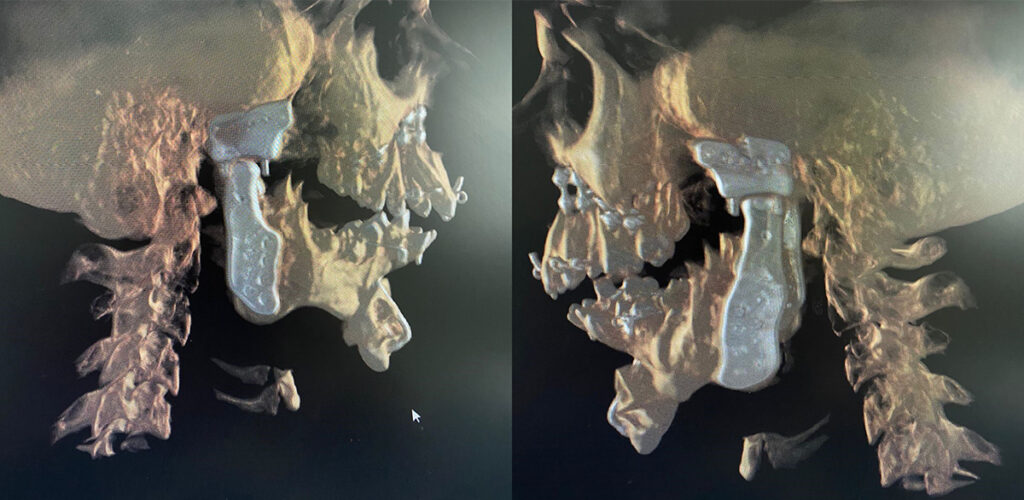
In the CT scan image shown here, you can see a large boulder-like enlargement of the joint. This is the ankylotic mass.
As the patient was in his teenage years, having completed most of his growth and having a severely deformed lower jaw, a temporomandibular joint reconstruction (TJR) with patient specific implants was planned for him on both sides.
TJR involves virtual surgical planning on specialised software and then 3D printing the patient specific implants.
The steps are listed as below:
Data acquisition- This is the first step in the process. It includes taking high resolution CT images to obtain an accurate joint picture and intraoral dental scans to get an accurate depiction of the patient’s bite.
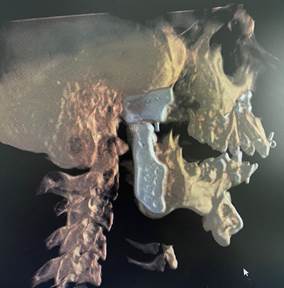
The second step is conversion of the imaging data into three dimensional digital models of the face.
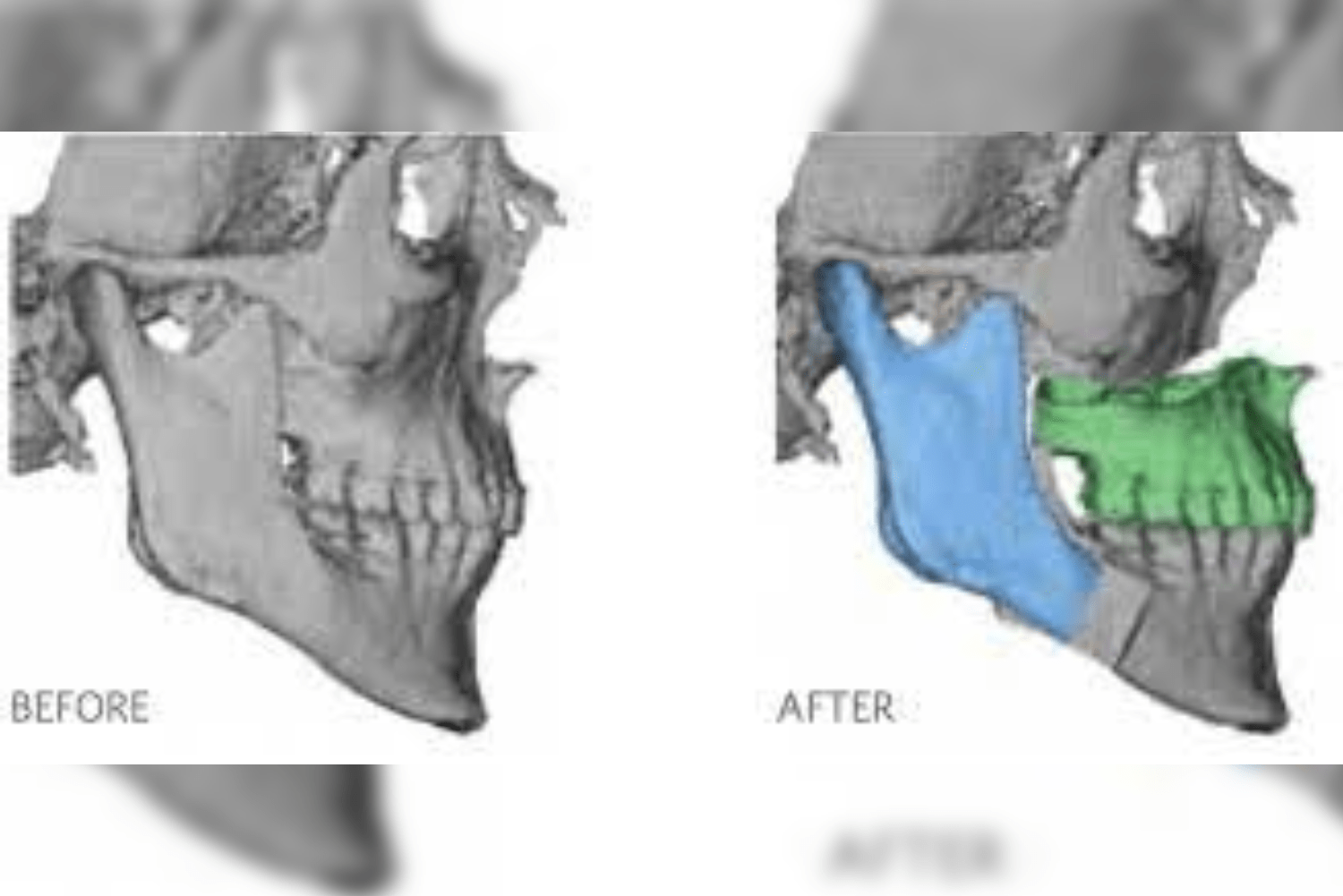
Once the 3D reconstructed models are obtained, the surgeon and the engineers simulate the surgical steps on the model. The ankylotic mass is removed and the prosthetic components are positioned digitally in the desired position replicating normal anatomy.
Based on the virtual surgical planning, the patient-specific implants are customised. Along with these implants, surgical guides are fabricated to aid in surgical precision and improved surgical time.
The last step includes manufacturing the implants using milling or additive manufacturing.
With the advent of patient-specific implants and virtual surgical planning, it is possible to treat such complex cases with surgical accuracy and reduced operative time which was deemed impossible to treat just a few years back and patients would have to undergo multiple surgeries at various stages of life.
These implants are made with medical grade titanium and are biocompatible, which means that they do not cause any foreign body reactions with the surrounding tissues of the body that they are fixed to. These implants are designed to bear heavy biting forces and to minimize the mechanical complications that might occur with constant, continuous use.
There are two parts to the PSI- the fossa component and the mandible component. The fossa component attaches to the cheek bone which is the fixed part of the joint and the mandible component attaches to the movable part of the joint that is the lower jaw. Together they function as one unit.

The surgical approaches used were: the pre-auricular approach (in front of the ear) and the perimandibular approach (from below the lower jaw) on either side, through which the fossa and mandibular components are fixed onto the bone. Such surgeries usually span from 6-8 hours and thus it is imperative to maintain a sterile environment with strict asepsis at all times to prevent any post-operative infection.
Below are the post-operative photos of the patient on the 8th day post surgery, with the surgical scars noted in the preauricular and perimandibular regions. A marked improvement in his mouth opening from literally one finger mouth opening to around 30mm post surgery was achieved. Along with this, a drastic improvement in his profile is seen.



Orthognathic surgery along with the placement of patient-specific implants is usually necessary in such patients. The upper and lower jaws are moved forward along with a counterclockwise rotation of the lower jaw to achieve optimal aesthetic results.
The post-operative CT scan showing the temporomandibular joints on both sides and the titanium miniplates used for fixation of the upper and lower jaw after bijaw orthognathic surgery.


Advantages of patient-specific implants:
- Improved accuracy
- Predictable outcomes
- Reduced surgical time
- No additional need to harvest bone from another site
- Improved long term stability
- Simultaneous orthognathic correction of the major facial deformity
Disadvantages of patient-specific implants:
- Cost
- Risk of prosthetic infection or mechanical failure, although rare
- Not suitable in children
Post-op care:
Patients are advised a soft diet for several weeks and strictly advised to avoid crowded areas for infection prevention in the first few days post surgery. Mouth opening exercises are to be followed early on with regular physiotherapy sessions. The patient is kept on regular follow up visits to monitor the joint function and uptake.
Conclusion:
We couldn’t be more happier seeing the results achieved with this patient and improving his functional ability and quality of life. With the advent of technology, the customised temporomandibular joint reconstruction is likely to become the standard of care in the future.