Obstructive Sleep Apnea (OSA) is a common sleep disorder where breathing repeatedly stops and starts during sleep. It’s not just heavy snoring; it’s a serious
TMJ also known as TEMPOROMANDIBULAR JOINT plays a crucial role in our day-to-day life. It helps us in performing various functions like eating, chewing, talking,
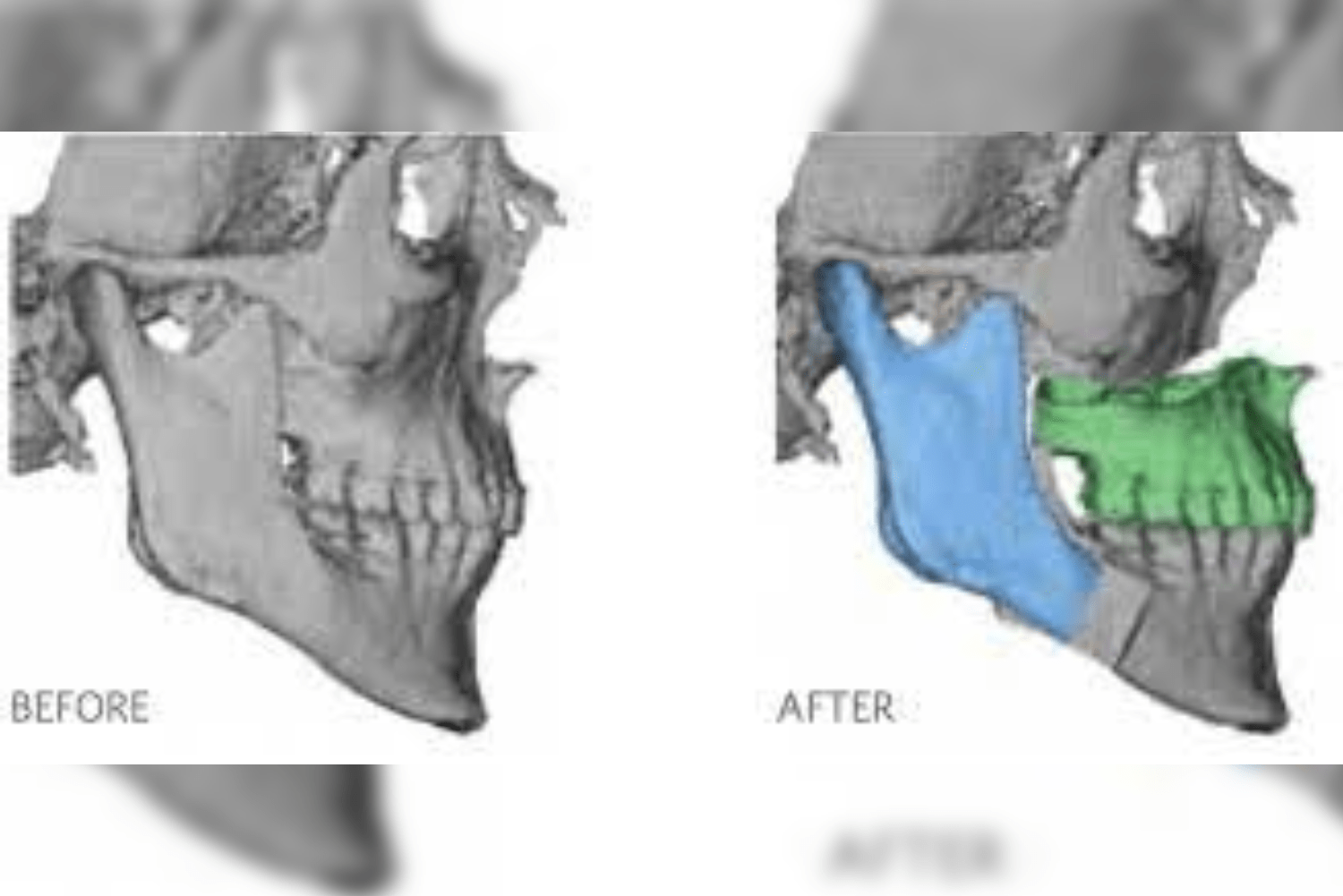
Temporomandibular Joint (TMJ) ankylosis is a serious disorder characterized by restricted jaw movement, pain, and frequently noticeable facial asymmetry. It is caused by aberrant bone or
The most effective treatment for obstructive sleep apnea (OSA) is continuous positive airway pressure (CPAP). But more than 50% of people cannot handle this procedure
Obstructive sleep apnea occurs when the airway partially or completely collapses repeatedly throughout the night. This results in breathlessness, causing the person to wake up long
Temporomandibular joint (TMJ) implants are intended to be surgically implanted in the jaw to replace the temporomandibular joint. A variety of artificial materials have been
Hearing Aids Treatment: What Is A Stapedotomy? It is the surgery that treats hearing loss or hearing impairment by removing a dysfunctional small piece of
What Does Voice Feminization Surgery Mean? Amongst the many gender affirmation surgeries, Voice Feminization Surgery is one which is done to make the voice more