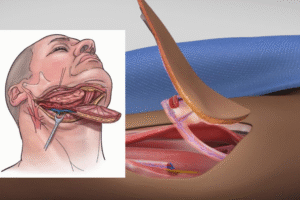
Introduction-Zygomatic Dental Implants Zygomatic implants are dental implants inserted deep into your upper jaw for the rehabilitation of the atrophic...
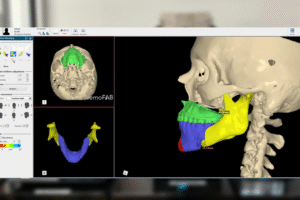
3D Printing in Healthcare has transformed the way industries like healthcare, automotive, manufacturing, and design operate. 3-D labs have revolutionised...