Abstract
Traditionally, observation has been the mainstay of therapy, with the expectation that most of the lesions will disappear spontaneously. This treatment plan was based on the premise that surgical excision or other treatments might produce a worse result than simply waiting for the lesion to resolve with an acceptable cosmetic result. This article presents a comprehensive Analysis of hemangioma treatment through various cases of face and neck hemangioma and evaluates the possibility of surgical excision as a first-choice treatment in these cases.
Pre- and postoperative photographs were examined. Hemangioma location, size, and type; patient’s age; and surgical technique are described. Acceptable cosmetic and functional results were achieved in all surgical cases, supporting the relevance of this Analysis of hemangioma treatment.
Clinical Data:
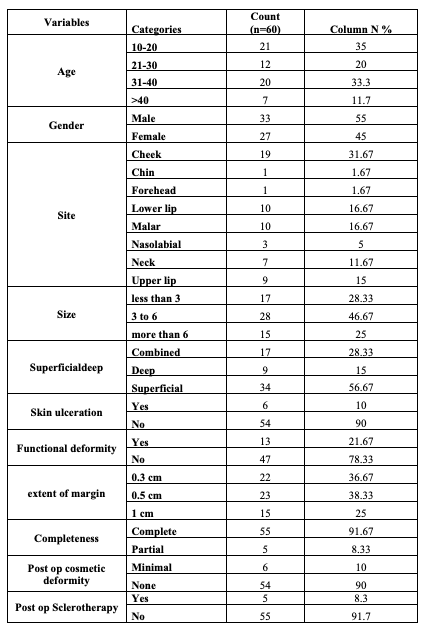
This was a retrospective study approved by the Ethics Committee at Richardson Face Hospital. All the patients signed the informed consent form. Patients’ medical records were maintained anonymous, and informed written consent was also obtained for publication of their cases and images. We collected data of 60 patients operated at Richardson Face Hospital with Face and Neck Hemangiomas between March 2024 to September 2024. Among these, 33 were males and 27 were females.
The age distribution was as follows:
-
Below 10 yrs – 17
-
11 to 20 yrs – 22
-
21 to 30 yrs – 13
-
31 to 40 yrs – 7
-
Above 40 yrs – 1
Most commonly, hemangiomas were seen between the age group of 11 to 20. This can be understood as most hemangiomas in infancy undergo a proliferative and involution phase. This section provides important clinical insights that support the broader Analysis of Hemangioma Treatment being carried out in this study.
Overall, the findings emphasize the need for age-specific evaluation in managing these cases, further contributing to the ongoing Analysis of Hemangioma Treatment in the face and neck regions.
Analysis Of Hemangioma Treatment
Hemangiomas are benign vascular tumors composed of proliferative, plump, endothelial cells. They can occur in skin, mucous membranes, and other soft tissues. The tumor may begin in subcutaneous tissue or muscle or may infiltrate the skin densely without elevating it, giving an appearance similar to that of a Port wine stain. Hemangioma typically present with both a superficial component and a deep cutaneous component as well as a subcutaneous proliferation of ectatic vessels. Several theories have been proposed, of which Folkman Klagsbrun placental theory, endothelial progenitor cell theory, hypoxia theory, and angiogenesis theory are the most accepted. This is an important part of the Analysis of Hemangioma Treatment.
Surgical approach to hemangiomas are more complex with age. In an involuting lesion, the hemangioma is a mixture of fibrofatty tissue and blood vessels and hence becomes very difficult in many of these lesions to distinguish between the hemangioma and normal tissue. As a consequence, this requires resection of a greater volume of normal tissue. Patients continue to present with lesions that cause permanent disfigurement after previous reassurances and only follow up with serial observations. Such cases are included in the Analysis of Hemangioma Treatment.
Hence it becomes pivotal to assess the feasibility of complete surgical resection and opt for surgical excision at first time of its presentation. This careful planning ensures optimal outcomes and forms a critical component of the Analysis of Hemangioma Treatment.
Objective:
Case Series:
A total of 60 cases of face and neck hemangiomas were studied and operated. The pattern of presentation of hemangiomas in face and neck studied and following observations documented. Diascopy was done in all cases to distinguish the vascular lesions from purpura. PHACE syndrome is considered in hemangiomas larger than 5cm. This forms an important part of the Analysis of Hemangioma Treatment.
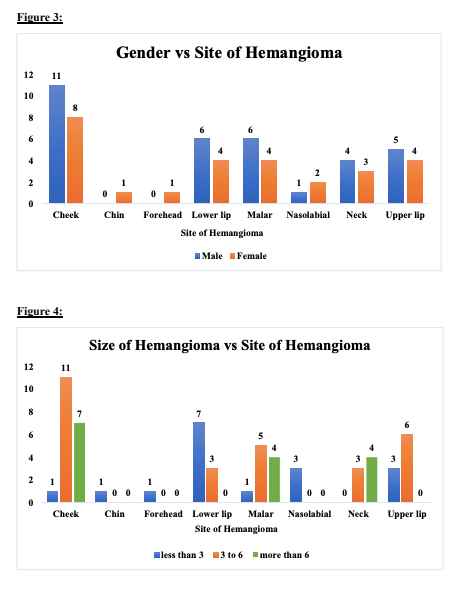
Size and Location of Lesion:
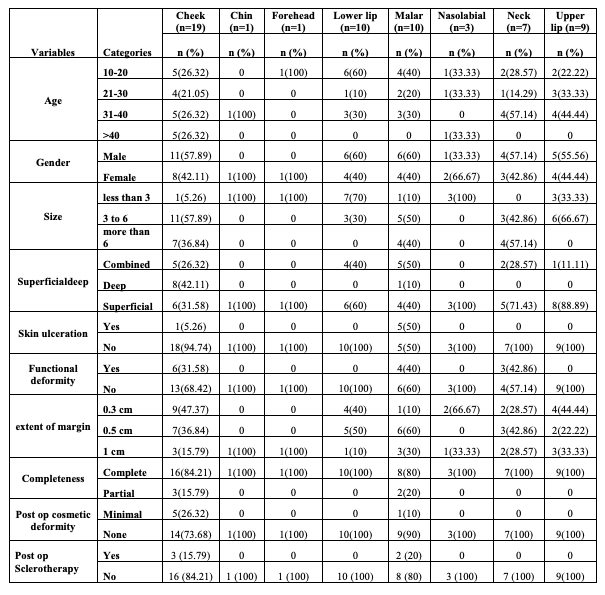
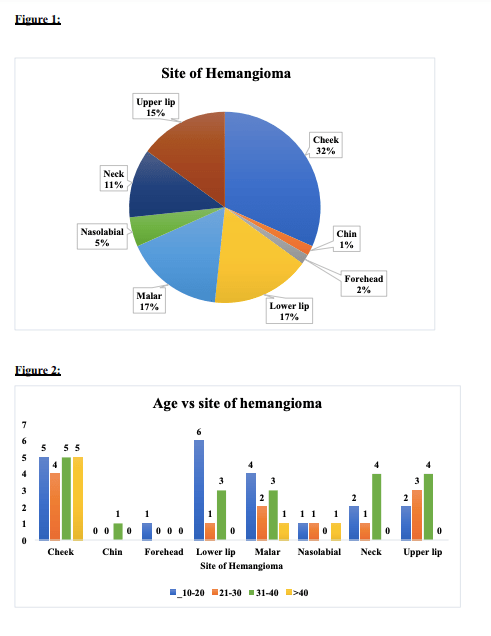
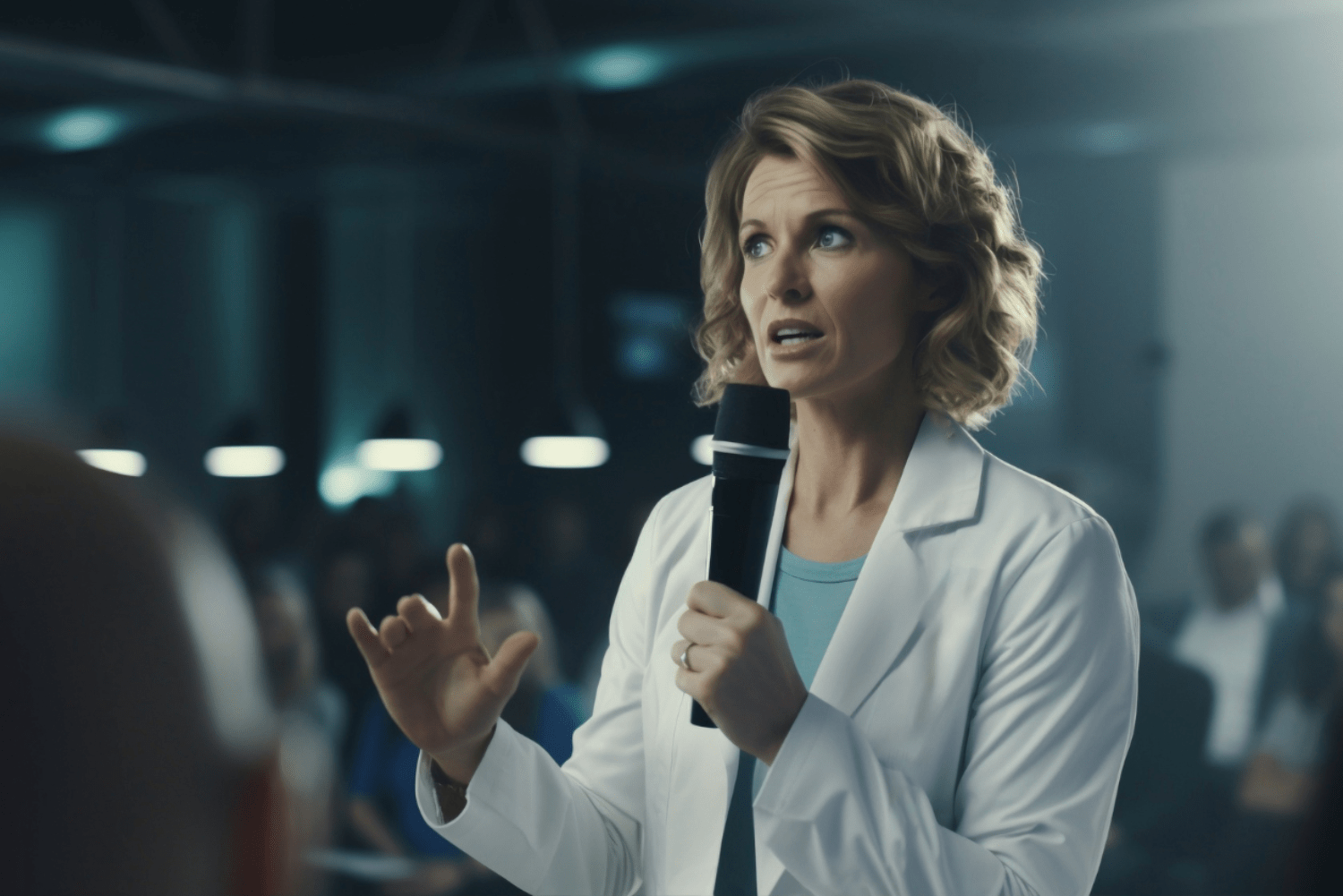
The size and site of hemangiomas and pre-operative assessment becomes pivotal for the extent of surgical clearance that can be achieved. They most commonly have been found to present over the upper lip 10%, lower lip 14%, mouth buccal 23%, malar region 8%, and eyes 5%. Most of them presented with both hindrance to functionality as well as cosmetic concern. Very small hemangiomas may not present with port wine stain. Hemangiomas that present in the eyelid can enlarge and eventually affect the visual axis. Those in the nose may impose problems due to rapidly enlarging lesions and cause deformity of the nose known as “Cyrano nose,” which means the underlying architecture of the nose is affected and requires surgical reshaping. Labial hemangiomas cause distortion of the vermillion border, posing a challenge during resection and resuturing. This assessment is crucial in the Analysis of Hemangioma Treatment.
Surgical Nuances:
Hemangiomas may not always look or present like typical hemangiomas. This variation can be attributed to the time course of presentation or the growth phase of the lesion. It is seen most frequently in rapidly involuting congenital hemangiomas. During the proliferative phase, the rapid growth of the lesion results in the formation of a “pseudocapsule,” which provides a very clear delineation between the lesion and the surrounding subcutaneous fat. Surgery to excise this can be essentially bloodless if one remains in this plane, making precise technique crucial in the Analysis of Hemangioma Treatment.
Lip Hemangiomas
Amongst 24 cases of lip hemangiomas, lower lip hemangiomas were found to be more common and mostly central in location. LIP HEMANGIOMAS notoriously have the tendency to cause ulcers, which eventually lead to scarring, hindering the overall post-operative outcome. Henceforth, it becomes pivotal to consider two main criteria:
-
Placement of scar: In order to restore the proper contour and outline of the lip, it is always better to place or extend the scar into the oral mucosa rather than the skin or vermillion border.
-
Central fullness and tubercle of lip: It is always imperative to maintain the central fullness, which is also the fullest part of the lip. Hence, while placing sutures, they were taken to create the labial tubercle.
This careful planning is crucial in the Analysis of Hemangioma Treatment to ensure optimal functional and aesthetic outcomes.

A case of lower lip hemangioma with distorted lip architecture



Clockwise:
a) Patient with a large lower lip hemangioma
b) Incision marking including 0.3 mm of normal surrounding skin
c) Extirpation of hemangiomatous tissue



a) Hemangioma of upper lip, lip contour maintained
b)removal of hemangioma and
c) close approximation of skin with 5’0 ethilon
Cheek Hemangiomas:
Among 23 cases of cheek hemangiomas, demonstrating varied depth, superficial lesions showed prominent port wine (red hue) which could be easily classified as lobulated or sessile, whereas deeper lesions were more difficult to visualize and appeared soft blue or with violaceous discoloration from surrounding mucosa. Among these, 12 patients were on beta blocker therapy for more than 6 months and 2 were on oral steroids which, however, did not improve symptoms or appearance and came to our hospital for surgical treatment. Most commonly encountered complications with oral hemangiomas were identified in this Analysis Of Hemangioma Treatment:
-
Speech impairment
-
Dysphagia
-
Hemorrhage
Surgical nuances: While considering cheek hemangiomas, approaches were made intraorally for superficial ones. Care was taken to tease off the lesion from the underlying muscle and avoid injury to the buccal branch of the facial nerve. For deeper lesions, the approach was made externally and closed in two layers to avoid seroma. Importance was given to maintaining the structural integrity of the muscle and nervous innervation of the cheek over the completeness of removal of the lesion. This forms an essential part of the Analysis Of Hemangioma Treatment.
Through detailed observation, the overall Analysis Of Hemangioma Treatment demonstrates that even after prolonged medical therapy, surgical intervention can provide definitive results, restore function, and improve cosmetic outcomes in cheek hemangiomas.



Cheek Hemangioma In the Deeper Plane



Malar Hemangiomas:
Hemangiomas arising or extending into the malar region were mostly mixed in origin—some superficial and some subcutaneous or deep hemangiomas arising from the reticular dermis and/or the subcutis layer. Most cases involved skin breakage and open sores, which could become infected. They could also extend medially and superiorly, causing pressure on the orbit, potentially leading to diplopia or even blindness. The approach to malar hemangiomas was mostly external to address ulcers and puckered skin. This is an important consideration in the Analysis Of Hemangioma Treatment.





Post Operative Outcome:
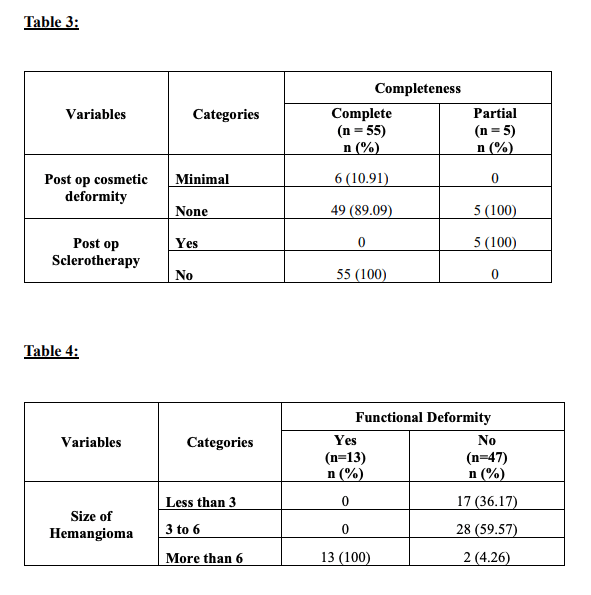
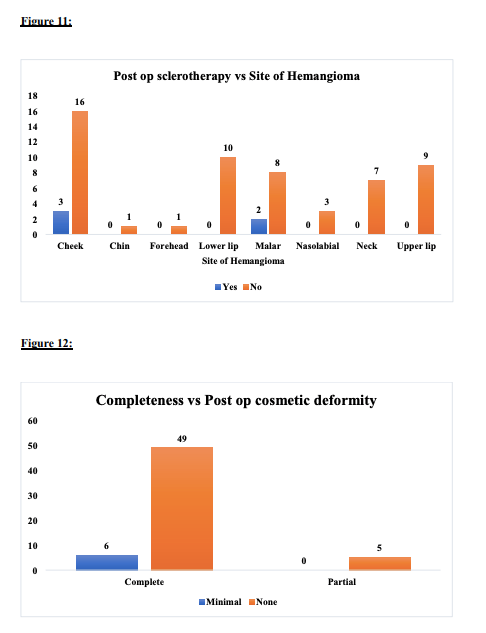
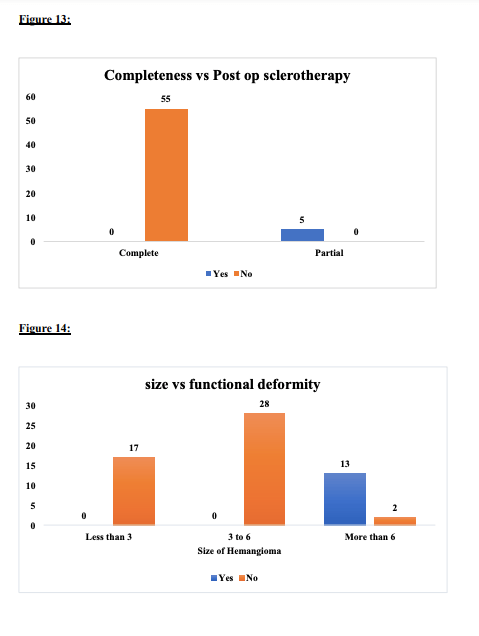
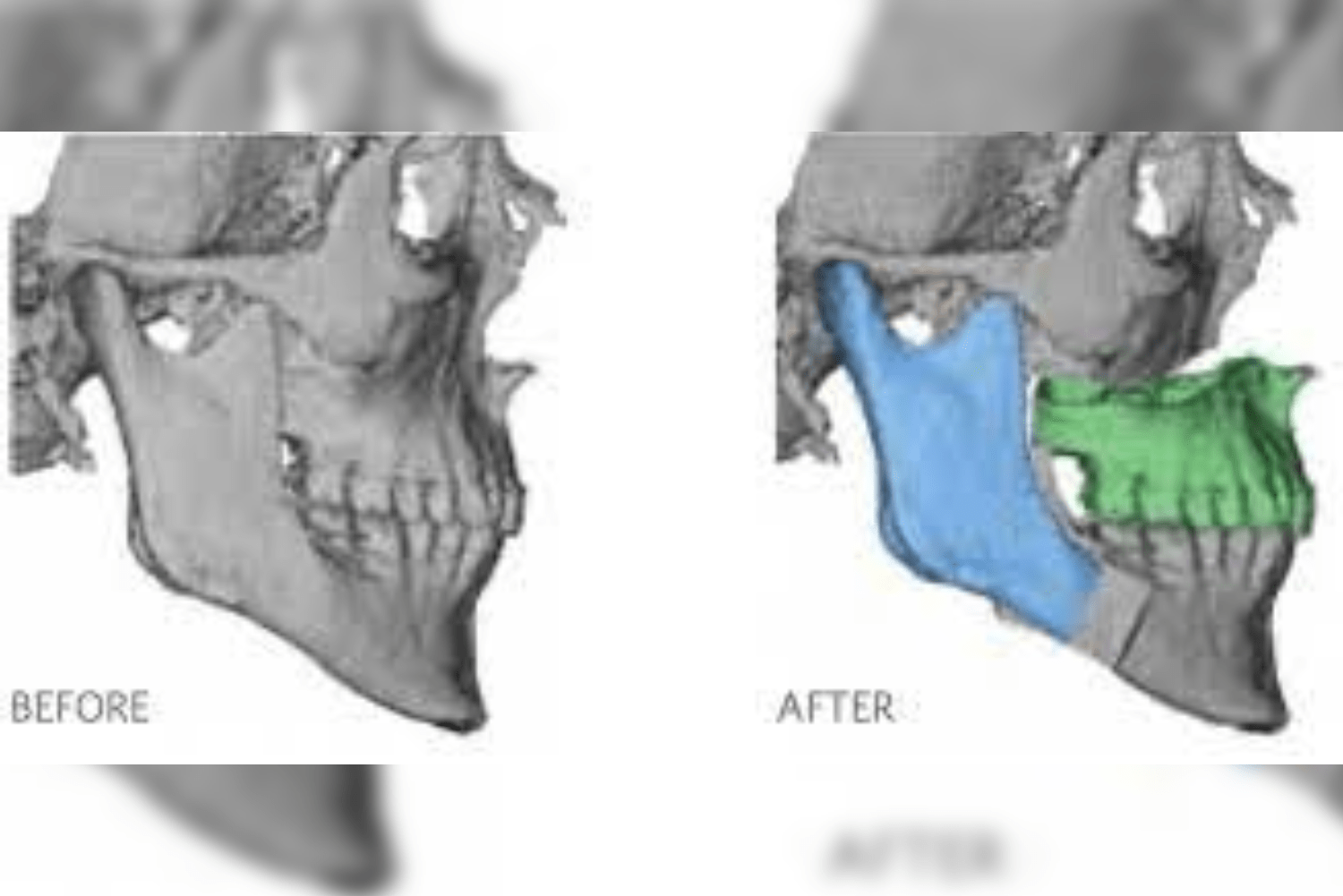
All patients were discharged on post-operative day 5, and sutures were removed on day 7. All operated patients are under follow-up. During the postoperative follow-up period, most hemangiomas (95%) maintained a stable morphology, showing no increase in growth. The overall shape of the lip and cheek was satisfactory. Two patients underwent postoperative sclerotherapy at 9 and 13 months after surgery. The sclerosant used was sodium tetradecyl sulfate, interlesionally injected with a 25-gauge needle at multiple sites, and the procedure was repeated after 2 weeks. This reflects the effectiveness in the Analysis Of Hemangioma Treatment.



Conclusion:
Historically, hemangiomas were managed with a watchful observation approach, assuming spontaneous involution, and active management was reserved for “complicated” cases. Currently, various medical and surgical options are available for the treatment of hemangiomas. Established treatments include intralesional bleomycin, corticosteroids, interferon-α, laser therapy, cryotherapy, and surgical excision.
Early excision of hemangiomas should be considered the procedure of choice in selected cases, particularly when medical management with beta blockers or steroids has failed. Hemangiomas located in areas where significant cosmetic or functional defects may occur should have surgical excision considered as first-line treatment. Preoperative classification of lesions was done according to the ISSVA classification of vascular tumors. Our modification involves coding the lesions based on size and depth, referred to as the Modified ISSVA classification of hemangiomas, which aids in effective Analysis Of Hemangioma Treatment.
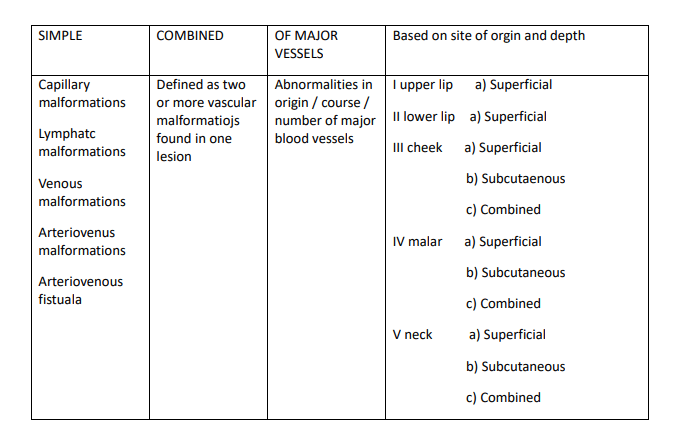
Based on this modified classification of hemangiomas, the site and depth can be assigned preoperatively to plan the approach and extent of dissection. This system allows for a more precise Analysis Of Hemangioma Treatment, helping surgeons choose the optimal surgical technique and anticipate potential complications it can be.
References:
Boyd VC, Bui D, Naik B, Levy ML, Hicks MJ, Hollier L Jr. Surgery: The Treatment of Choice for Hemangiomas. Semin Plast Surg. 2006 Aug;20(3):163–8. doi: 10.1055/s-2006-949118. PMCID: PMC2884763.
Enjolras O, Borsik M, Herbreteau D, Merland JJ, Hadjean E, Tran Ba Huy P. Indications chirurgicales dans les angiomes de face [Surgical indications in angiomas of the face]. J Chir (Paris). 1993 Oct;130(10):416-21. French. PMID: 8276910.