Facial Types
The field of Orthognathic surgery has been an ever advancing speciality striving to restore the facial harmony by surgical transformation of facial types. The facial types have been classified by various authors as the following
Graber (1988) described three facial types
- The brachycephalic is likely to have a broad dental arch to go with the broad facial structure;
- The mesocephalic probably have an average dental arch form
- The dolichocephalic is most likely to have a long and narrow dental arch to harmonize with the long and narrow face.
Farkas and Munro (1987); Proffit (1991); Salem (2003)
(fig:5) Have determined facial types, by calculating the ratio between interzygomatic distance and anterior facial height, then the face type for each subject is classified as follows:
- Euryprosopic (Short & Broad Facial Type) – The facial index is > 0.93
- Mesoprosopic (Medium Proportional) – The facial index is ≤ 0.93 and ≥0.83
- Leptoprosopic (Long and Narrow) – The facial index is<0.83

(Broad Face Type)

(Average Face Type)

(Tall, Narrow Face Type)

Euryprosopic Facial Type
Euryprosopic facial type is broader and shorter, and frontally appears flat or shallow. It is also characterized by: wide-set eyes; a short, rounded “pug like” nose, with straight or convex bridge and an upturned nasal tip; an upright bulbous forehead; and prominent cheekbones. This facial type corresponds to the brachycephalic headform.

Mesoprosopic Facial Type
Mesoprosopic facial type is the more neutral and lies between the leptoprosopic and Euryprosopic facial types.

Leptoprosopic Facial Type
Leptoprosopic facial type the face is narrow, long and protrusive. The eyes are closely set, the forehead is sloping, the supraorbital rims are prominent, and the nose is thin, long and protrusive. This facial type corresponds to the dolichocephalic headform.
Clinical Examination – Extraoral Examination
1. Assessment of Facial Thirds

The face is divided into 3 parts:
- Upper one third (Trichion to Glabella)
- Middle one third (Glabella to Subnasale)
- Lower one third (Subnasale to Menton)
The patient is checked for the proportionality of the face. Mesoprosopics have the face divided into equal one thirds whereas euryprosopics have deficient lower one third and leptoprosopics have vertically increased lower one third.
2. Evaluation of Vertical Facial Fifths
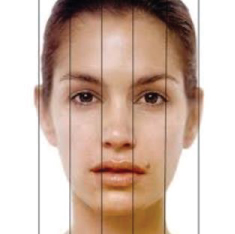
In this criteria the horizontal width of the face is divided into five vertical equals.
This assessment helps determine any facial dysmorphias or assymetry that exists.
3. Check for Facial Asymmetry
The face of the patient is assessed for any mandibular deviation, chin point displacement and midline discrepancies which might complicate the surgical planning.
4. Lip Competence at rest
Lip competence is a key feature for the clinician to arrive at a diagnosis. for long face patients, the lips remains apart even at rest . on the contrary, the lips seem closed and everted for euryprosopic.
5. TMJ Evaluation
TMJ examination is quintessential for surgical planning. The patients are checked for any clicking, crepitus, dislocations,deviations of the TMJ joint.
Intraoral Examination
Occlusal Assessment
1. Angle Classification
Leptoprosopic patients may have class II malocclusion, that is a small and retrognathic mandible or a prognathic maxilla.
Euryprosopic patients may have class III malocclusion with mandibular prognathism .
2. Overjet and Overbite
Deep bite are usually seen in euryprosopic patients and open bite is seen to be associated with leptoprosopic or high angle cases.
3. Transverse Discrepansies
Conditions such as cross bites, scissor bites, brodie bites can disrupt the functionality of the jaws and enhance inefficiency while chewing.
4. Periodontal health and Alveolar bone levels
Good periodontal health and average bone levels allows the teeth to be strong and intact in the mouth.
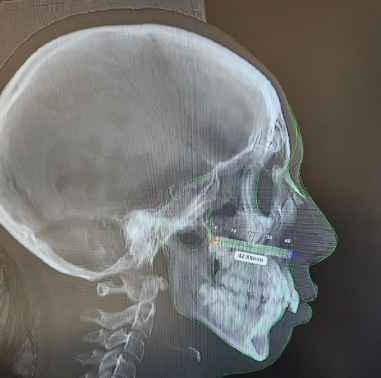
Cephalometric Evaluation
Cephalometric evaluation is a crucial diagnostic tool that uses standardized lateral skull radiographs to analyze the relationship between bony, dental, and soft tissue structures. It enables precise diagnosis of jaw discrepancies, evaluation of growth patterns, and the planning of surgical cases.
Burstone and Legan – Cephalometrics for Orthognathic Surgery Analysis
COGS analysis is considered the backbone for surgical planning. Its an analysis designed for patients requiring orthognathic surgery given by Burstone and Legan for hard tissues in the year 1978 and in 1980 for soft tissue analysis. Burstone and Legan were internationally recognized Orthodontic experts in diagnosis of orthognathic cases, obstructive sleep apneas and distraction osteogenesis.
COGS Hard Tissue Analysis 1978
The analysis includes:
Cranial base measurements
This illustrates the position of maxilla and mandible wrt to the cranial base.
Horizontal skeletal and dental profile
Horizontal relationship of the facial structures are studied . the analysis signifies if the maxilla and the mandible are prognathic or retrognathic.
Following parameters are studied
- Horizontal position of maxilla wrt cranium
- Horizontal position of mandible wrt cranium
- Antero-posterior relationship of maxilla to mandible
Vertical skeletal and dental profile
This analysis quantifies the vertical deficits or excess in the patient which translates as an antero-posterior facial dysplasias.
It discusses about
- The height of middle anterior face
- The height of middle posterior face
- The height of lower anterior face
- The height of Ramus
- Vertical length of chin.
After studying the above findings, it allows the treating surgeons to know exactly how much milimeters of corrections does the patient require to restore the facial proportionality in turn enhancing aesthetics.
Maxilla and mandibular relations
The analysis in this category helps differentiate which structure of all is at fault in particular. Here each structure is studied individually as well as the extent to which the relationship of the structures is derailed is studied.
Following parameters are studied
- Length of maxilla
- Length of mandible
- Relationship of maxilla with mandible
- Gonial angle
- Mandibular angle.
Transforming Leptoprosopic Facial Type – Reduce The Vertical Excess
Leptoprosophic facial type also known as long face syndrome presents with the following features:
- Long and narrow face.
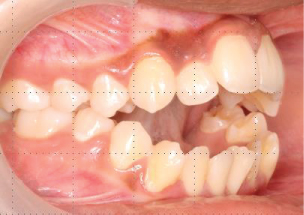
- Anterior open bite, often.
- Present as skeletal class III
- Increased lower face height.
- Gummy smile
- Vertical growth pattern
- Long and narrow dental arches
- Lip incompetence

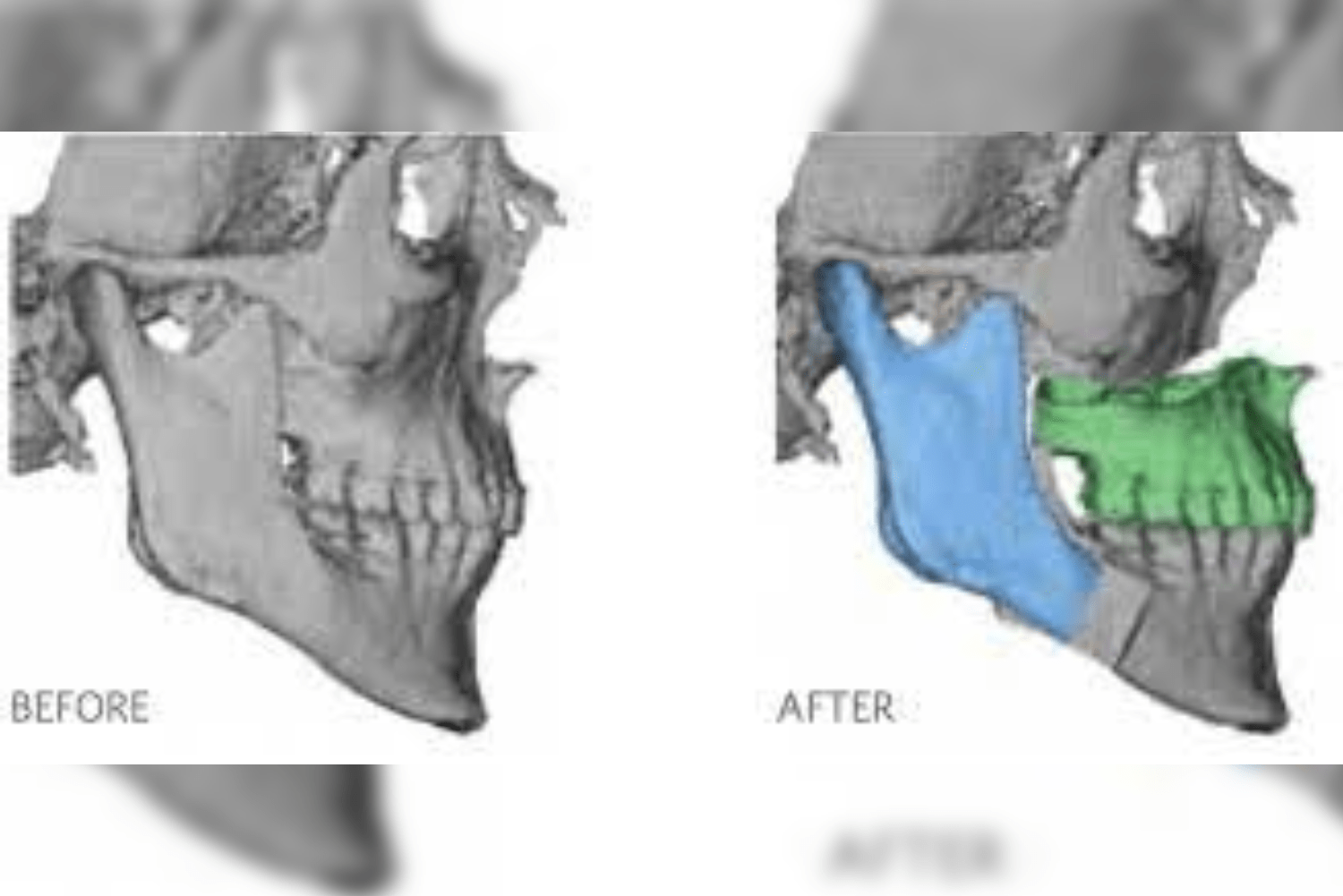
Case of anterior open bite, associated with long face syndrome.

Surgical Techniques for Correction
Transforming a leptoprosopic face towards mesoprosopic proportions demands for reduction of the vertical face height through the following ways:
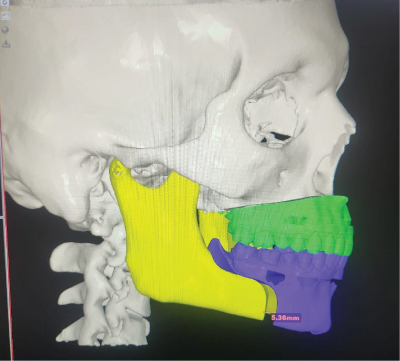
1. Maxillary Impaction (Le Fort I with Superior Repositioning)
A surgical procedure that involves superior positioning of the maxilla, as a result of which the mandible auto rotates counter clockwise upwards,effectively reducing the lower facial height.

2. Mandibular Height Reduction
Studies show that leptoprosopic patients achieved vertical correction primarily through mandibular height reduction- whether by mandibular setback, counter clockwise rotation of the maxillomandibular complex, or genioplasty.
3. Combined Maxillomandibular Surgery (3-Jaw Surgery)
The most predictable approach often involves simultaneous:
- Le Fort I osteotomy
- Bilateral sagittal split osteotomy (BSSO)
- Genioplasty
This combination allows precise control over all three dimensions and permits both vertical reduction and anteroposterior correction
Transforming the Euryprosopic Face: Addressing Width and Height
The Problem
Euryprosopic patients present with:
- Broad, short facial appearance
- Prominent bizygomatic width
- Reduced lower facial height
- Often associated with deep bite
- May have skeletal Class II features
Surgical Strategies
Converting a euryprosopic face toward mesoprosopic proportions is arguably more challenging because it may require:
1. Vertical Lengthening Procedures
- Maxillary downgrafting: Moving the maxilla inferiorly with interpositional bone grafts
- Mandibular advancement with counterclockwise rotation: This effectively increases lower facial height
- Genioplasty with vertical lengthening
2. Width Reduction (When Indicated)
- Zygoma reduction osteotomy: Narrowing prominent cheekbones
- Mandibular angle reduction: Addressing a wide gonial angle
3. Combined Approaches
As with leptoprosopic transformation, three-jaw surgery provides the most control. The movements differ—instead of impaction and setback, the surgeon may employ:
- Maxillary downgrafting
- Mandibular advancement
- Counterclockwise rotation of the occlusal plane



Conclusion
Transforming a leptoprosopic or euryprosopic face into a mesoprosopic ideal is one of the most demanding yet rewarding challenges in orthognathic surgery. It demands an accurate clinical examination, rigorous cephalometric analysis using Burstone’s and Legans hard and soft tissue norms which culminates into a systematic planned surgical and orthodontic plan tailored to each patients unique skeletal pattern.
For Leptoprosopic patients- the goal is to reduce the vertical skeletal excess by either lefort I maxillary impaction and autorotation of the mandible.
For Euryprosopic patients- the focus shifts to increasing the vertical dimension by lefort I inferior repositioning and rotating the mandible downwards and backwards.
Hence, Orthognathic surgeries are striving towards restoring the facial proportion.
Richardson Hospital
Richardson Hospital in Bangalore offers all Orthognathic procedures