Burn injuries are a significant health issue and are a leading cause of accidental death or injury in India. Burns to the face can affect many specialised structures that are critical to survival and human function to include the mouth, nose, eyes, and ears. Beyond the functional aspect of facial burns, the aesthetic component is critical as we interact with the rest of the world with our faces.
Contractures and hypertrophic scars are two frustrating sequelae of thermal injury. Scars of the face and neck region are prone to be unusually severe because:
1. Its skin is rather loose, thin and thus easily destroyed
2. The area from the chin to the sternum is a concave flexor surface.
3. The extreme mobility of the neck makes it prone to contracture formation.
4. Vertical incisions in the skin of the anterior cervical area, whether accidental or surgical, are likely to result in contracted scar bands.
Other than burn scar and contracture, these patients are completely healthy and successful reconstructive surgery can often restore them to a happy and productive life. Patience, persistence, and determination are essential to accomplish successful reconstruction. The ultimate principle of reconstruction of post-burn neck contracture is learning to understand, appreciate and favourably influence the process of wound healing & scar maturation.
Patients with facial burns present the clinician with the challenge of treating both functional and aesthetic needs. At its most basic, the face is needed for breathing and oral intake. It is also remarkably complex in its anatomy, providing us with sight, hearing, and smell.
Facial burns have many long-term physical, psychological and social sequelae. They require a healthcare team approach to management, which could last months to years.
Burns injuries can be the result of thermal (flames, hot liquid, contact with hot surfaces), or non-thermal (electrical, chemical, friction or radiation) contact.
The treatment of facial burns aims to:
- Pain control
- Address inhalation injury
- Encourage movement and function
- Oedema Management
- Tissue repair
- Scar Management
- Patient education
- Exercise regimen
- Optimize psychological well-being
- Cosmetic optimization.
- Optimizing the individuals’ self-management of scar tissue
If a patient is able to comply with physiotherapy and occupational therapy advice in the long-term, this can make a huge difference to the overall outcome.
The skin in made up of a number of layers:
- Epidermis: Superficial layer which is avascular
- Capable of regeneration. However, cannot regenerate if a large portion of this layer is destroyed.
- Dermis: Deeper, thicker layer of connective tissue
- Contains blood vessels, nerves, glands and hair follicles.
- Subcutaneous tissue: Deep, contains areolar and adipose tissue
- Contains large blood vessels, fat cells and connective tissue overlaying muscle and bone.
A first-degree burn damages the epidermis, a second-degree burn will also damage the dermis layer, and a third-degree burn is deep and damages the subcutaneous tissue. The depth of the burn will affect the risk of skin pigmentation, risk of scarring and also the length of time to heal.
Healing Timeframes Post-Burn Injury
| Table adapted from Glassey 2004 |
| Degree | MOI | Scar / contracture |
| 1st | Sun exposure, hot liquid (low viscosity) | None |
| 2a (superficial) | Hot liquids, chemical burns, flash | Minimal |
| 2b (deep) | Flame, electrical, hot liquid (high viscosity) | High risk |
| 3rd | Flame, electrical, chemical, blast | Severe risk |
| 4th | Prolonged exposure to flame, chemical, blast | Definite |
Oedema:
Your face and neck are at high risk of burns, as it is rarely covered by clothing or other protective gear.
However, there are protective characteristics that often reduce the depth of burn injuries to these areas :
- People tend to protect their face and shake/wipe off substances.
- Less likely to have materials over the face that could absorb the heat and increase time in contact with skin.
- Skin on face is relatively thick (except eyelids) with a good blood supply to dissipate heat.
Widespread complications of deep or widespread burns can include sepsis due to loss of barrier to infection, burn shock due to hypovolemia, vascular resistance, hypoperfusion and anti-inflammatory processes, as well as contracture due to formation of scar tissue. Burns can also lead to dehydration due to a loss of bodily fluids due to the death of skin cells.
Risks by area
The risks for body areas are:
Back of head: Area of thin skin with risk of exposure of underlying bone. It may also result in areas of alopecia.
Ears: Risk of exposure of the underlying cartilage, which is relatively avascular and at risk of infection.
Forehead: Less fat and muscle in this area can increase the risk of exposed bone.
Eyelids: Also thin skin and at risk of exposure of underlying tissue/eyeballs. They also provide little resistance to forces of contracture and are prone to forming ectropions, exposing the inner eyelid.
Eyes: Ocular burns may lead to infection or tissue ischemia. Chemical burns, particularly to the cornea, are an ophthalmologic emergency.
Nose: Risk of shrinkage of the nostrils and the nasal alae. Also at risk of exposure of underlying cartilage and bone, which are relatively avascular and at risk of infection. Singed nasal hairs may indicate inhalation injury.
Cheeks: This area has mobile, thick skin with good resistance to skin contracture. However, difficult to immobilise for healing post-surgery.
Lips: Prone to shrinkage or eversion as a result of contractures. Significant swelling of the lips or tongue may compromise the airway.
Neck: More prone to contractures in younger patients, due to reduced laxity. The skin loosens with age, creating more tolerance for shrinkage. Significant or circumferential burns may impact respiratory function or swallow, as well as the neurovascular systems.
Facial burn rehabilitation is of great importance in the whole process of facial burn management, leading to better outcomes of facial burns after decades of clinical experiences. With the development of rehabilitative theory and techniques, facial burn rehabilitation nowadays should include updated content and advanced methods, and a comprehensive rehabilitation plan is necessary to enhance the quality of facial burn management.
Initial rehabilitation before maturation of scars:
combination of silicone gel with pressure therapy
The combined intervention strategy of pressure therapy and silicone gel. The combination of silicone gel with pressure therapy has been shown to be more effective in providing benefits to the scar maturation outcome. It is also recommended by the ISBI Practice Guidelines Committee that all extensive burn hypertrophic scars should receive pressure therapy with silicone therapy as the first line of treatment.
Since the facial contour is complicated with individualised convex and concave surfaces, the combined pressure therapy with silicone gel for facial hypertrophic scars needs a more customised intervention strategy.
The 3D-printed transparent facemask with silicone linings is a promising solution for the effective application of the combined therapy. It has been used in our patients with favourable clinical results. But the patients need to maintain the treatment for at least half a year, until the maturation of the hypertrophic scars to achieve a stable clinical outcome.
Scar massage
Massage can increase the pliability of scarred skin, reduce pain, hypersensitivity and pruritus; therefore, is also recommended for facial burn rehabilitation, especially for cases that have already developed protruding hypertrophic scars and contracting scar bands. Massages are usually applied with emollients.
Techniques of massage mainly include Zig-Zag mobility, pinch and roll, traction, stretch, friction and circular mobility with different combinations.
Late rehabilitation after scar maturation
Morbidity related to hypertrophic scars and contractures, which are well-known sequelae after burns, remains high and, in fact, has increased as more severely burned patients are surviving. The goal in management is to restore the function and form of the origin.
Post-burn neck contractures not only affect the movements of the neck, but also can affect the function of the lower face, as well as result in possible tracheal alteration and distortion of the cervical spine. As these contractures cause major functional and cosmetic problems with resultant economic and psychosocial implications, operative correction is generally recommended, particularly in children in whom they can cause growth imbalance in the head and neck area.
The objectives of surgical intervention are to release the scar, restore cervical movements, appearance and natural profile and avoid recurrence of contracture.
Surgical procedures
- Z-plasty:
Z-plasty is a plastic surgery technique that is used to improve the functional and cosmetic appearance of scars. With this technique, it is possible to redirect a scar into better alignment with a natural skin fold or the lines of least skin tension. Contracted scars may be lengthened with this technique.
Z-plasty involves the creation of two triangular flaps of equal dimension that are then transposed. Basic z-plasty flaps are created using an angle of 60 degrees on each side, which can lengthen a scar by 50 to 70 percent and reorient the direction of the central wound by 90 degrees.
Keeping the length and angle of each flap precisely the same is key to avoiding mismatched flaps that may be difficult to close.
Some possible complications of z-plasty include flap necrosis, hematoma formation under the flaps, wound infection, trapdoor effect, and sloughing of the flap caused by high wound tension
- Skin grafting:
Skin grafting is a type of surgery. Your surgeon takes healthy skin from one part of the . body (preferably inner thighs) and transplants (move) it to the neck or face region.
The thigh skin usually matches the colour of your face and neck. The healthy skin covers or replaces skin that is damaged or missing on the inner thigh region. Skin loss or damage can result from burns, injuries, disease or infection. It is often used to cover broader contractures.
The recovery time after this surgery varies depending on your overall health, the size of the graft and the technique your provider used. Most skin graft procedures are successful the first time. Sometimes, the transplanted skin doesn’t heal well or “take” to the surrounding skin. If this happens, you may need another skin graft.
- Flaps: Flap surgery is a technique essential to plastic and reconstructive surgery. A flap is defined as tissue that can be moved to another site and has its own blood supply. This is in comparison to a skin graft , which does not have its own blood supply and relies on vascularisation from the recipient site.
Flaps have many uses in wound healing and are used when wounds are large, complex, or need tissue of various types and bulk for successful closure and function.
- Local flaps: Flaps taken from nearby tissue.
- Free flaps: A complex procedure where a flap is completely detached and reattached to the new site using microsurgery.
- Tissue expansion: Tissue expansion is a technique used by plastic, maxillofacial and reconstructive surgeons to cause the body to grow additional skin, bone, or other tissues.
Skin expansion is a common surgical procedure to grow extra skin through controlled mechanical overstretch. It creates skin that matches the colour, texture, and thickness of the surrounding tissue, while minimising scars and risk of rejection.[1]
When skin is stretched beyond its physiological limit, mechanotransduction pathways are activated. This leads to cell growth as well as to the formation of new cells. In some cases, this may be accomplished by the implantation of inflatable balloons under the skin.
By far the most common method, the surgeon inserts the inflatable expander beneath the skin and periodically, over weeks or months, injects a saline solution to slowly stretch the overlaying skin. The growth of tissue is permanent, but will retract to some degree when the expander is removed.
The excess skin is then used to cover the defect after the contracture is released.
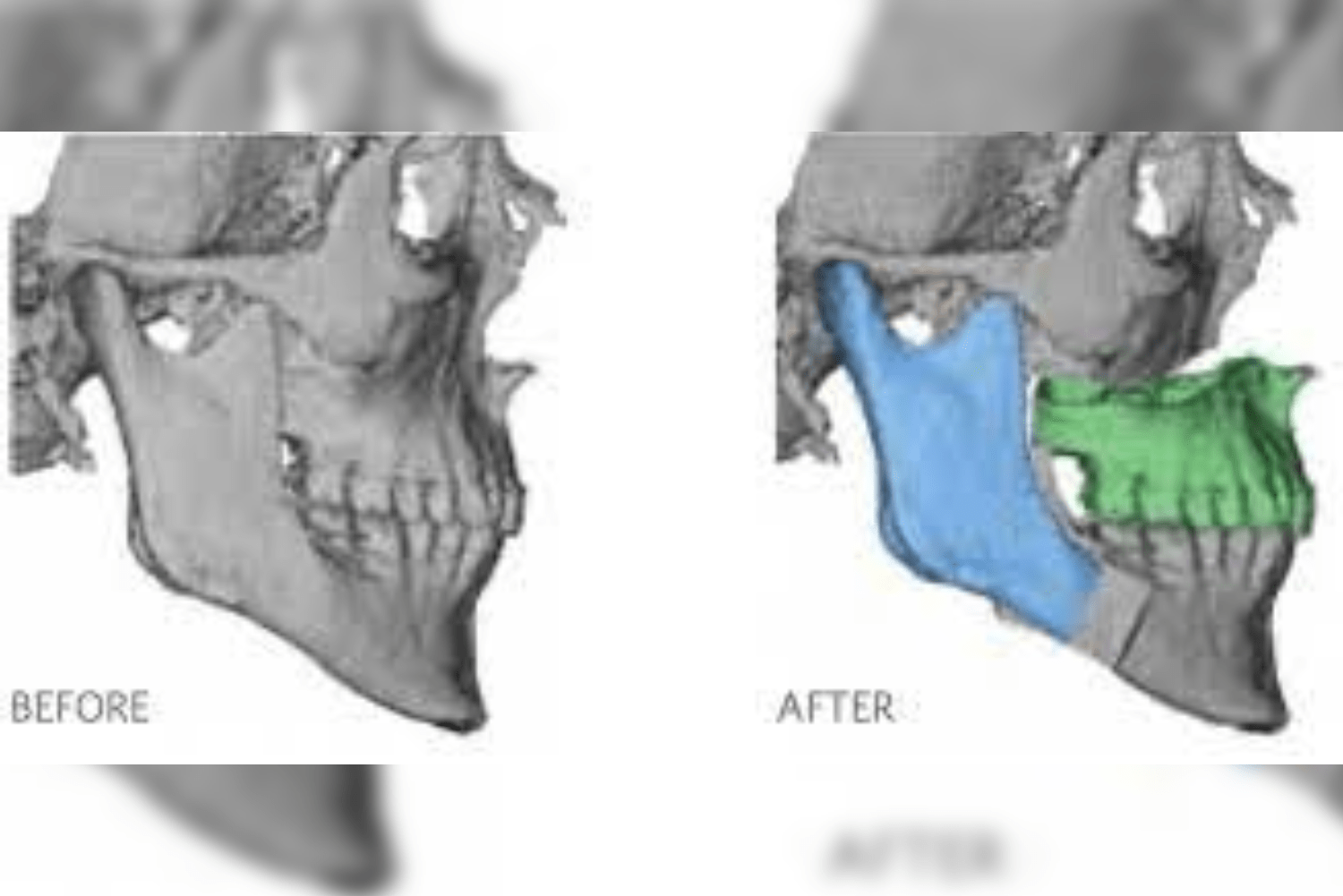
- Facial bone rehabilitation
In many of our post-burn status of patients, we have found that there is defined facial asymmetry due to bony reasons.
It is more obvious in patients who had burn injury in their growing years. This would prevent the bone not growing appropriately in the affected site. This hindrance leads to well obvious facial asymmetry which needs correction.
We have performed various types of jaw surgeries to correct the deformities.
Surgeries like genioplasty, maxillary impaction, bijaw orthognathic, and temporomandibular joint replacement surgery have been performed along with contracture release to provide an asymmetric and confident face.






- Lip reduction: burn injury patients often have thick lips due to venous derangement after burn scars. The venous drainage from the lips is not taken care of, and it bulges in sizes that make it look pretty off the dimensions.
Lip reduction surgery in them plays a vital role, leading to good aesthetic as well as functional results. It leads to the formation of a good lip seal.
- Other techniques:
Depending on the contracture type, other methods like double opposing Z-plasties or X-release can be used. Hypertrophic scars are managed with intralesional steroids and laser therapy.
Postoperative management
Patients were nursed in the supine position. When a flap is used, its temperature, colour and capillary blanching time are monitored and appropriate measures taken as necessary, in case of doubtful vascularity. In grafted patients, the neck is maintained in extension with a shoulder support. A small rolled towel or a blanket will be placed transversely beneath the neck. The dressing will be changed 5-7 days after surgery. At the next dressing, if the graft is well settled, local lubricating creams are advised.
Conclusion
Excision of all scar tissue is possible in severe contractures, but incisional release is required in extensive contractures. Skin grafting is a simple, reliable and safe operation, but has the disadvantage of hypertrophy and recurrence of contracture. Local and regional flaps provide a predictable reconstruction with a good colour and texture match, but may not be available because of severe scarring of the surrounding tissues. While post-operative neck function is essential, the cosmetic appearance is also equally important.